Medical Link Suzuki Frame Article
The Gold Coast Upper Limb Centre and Gold Coast Hand Therapy have joined forces to advance upper limb research on the Gold Coast.
Researchers Dr Michael Kalamaras (Orthopaedic Hand and Upper Limb Surgeon) and Kate Thorn (Hand Therapist) are reviewing patient outcomes after treatment with Suzuki Frame surgery for complex intra-articular fractures and dislocations in the finger.
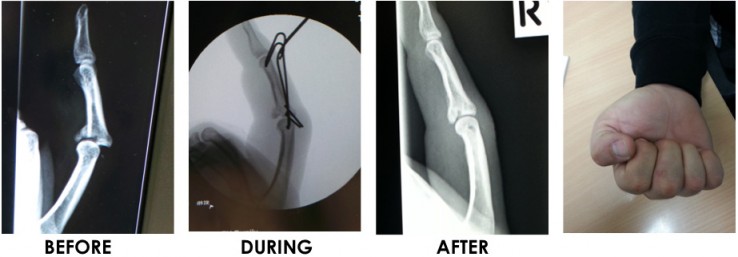
Dynamic traction external fixation, or the “Suzuki frame” is the brainchild of a Japanese hand surgeon, Dr Suzuki, who invented it in 1994. It is a finger traction system which a surgeon makes out of relatively inexpensive wires and dental rubber bands. It is inserted into the patients finger “percutaneously” or without any incisions, and can be performed as a day procedure. It allows the patient to move a heavily damaged finger joint whilst strong traction is maintained providing correction of the fracture whilst it is healing.
Suzuki frames are relatively well known around the world by specialty hand surgeons. In Australia, Suzuki frame traction is sometimes used when a fracture or dislocation is so severe that there are not many other options available. On the Gold Coast, Dr Kalamaras has performed this technique more than any other surgeon in Australia.
The Gold Coast study included 20 participants. Patients who underwent surgery with Dr Kalamaras between 2011 and 2015. The average age of participants was 37 years. The most common mechanism of injury was sports related (35%), split evenly between cricket and football. Other causes of injury were punch injuries, crush injuries and falls.
On average, patients underwent surgery within 11 days of injury.
Post-operatively, a hand therapist fabricated a custom-moulded thermoplastic splint to cover the hand and frame. This is particularly useful when the patient is sleeping or in public to protect the frame. The patient is able to perform flexion and extension exercises with the frame on to minimize adhesions during the healing process which optimizes range of motion after treatment. The frame is removed in theatre when evidence of radiological or clinical union is present, usually at 6 weeks. A manipulation of the joint is performed in most cases to release remaining adhesions and improve the range of motion further. The patient then attends hand therapy to regain movement and strength in the hand.
The mean active range of motion of the proximal interphalangeal joint (PIPJ) of the affected finger at follow-up was 86 degrees, compared to 99 degrees on the contralateral side. The mean grip strength of the affected hand was 47kgs, compared to 46kgs on the contralateral side (three quarters of participants injured a finger on their dominant hand). The average QuickDash score was 4.5. The average pain level at worst at final follow-up was 16 on a 100-point visual analogue scale, while at rest it was 2 out of 100. Participant overall satisfaction was 88 out of 100. All of the participants have returned to pre-injury work status.
The reported complications in this study were minor, including slight extensor lags and residual stiffness in the PIPJ, which is remarkable given the severity of the injuries treated. Few patients required a manipulation and tenolysis at a later stage.
If you would like to know more please contact Dr Kalamaras’ rooms on 07 5532 2721 or Gold Coast Hand Therapy on 07 5500 5617.