Dupuytren’s Disease
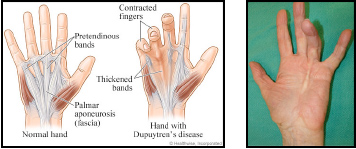
Dupuytren’s Disease is characterised by an abnormal thickening of the tissue just beneath the skin and initially appears as a firm nodule just under the skin in the palm of the hand. As the disease progresses, thick cords develop, extending from the palm into one or more fingers causing the finger/s to bend or contract in. It can affect both hands. The ring and little fingers are most commonly affected. Progression of Dupuytren’s Disease is unpredictable, with some individuals having only small lumps or cords while others will develop severely flexed fingers.
Surgery
The evidence suggests that surgical correction provides the most successful results for patients with this condition. Surgery involves removing the diseased tissue and releasing any structures which may have contracted/tightened during the disease process to allow full movement of the joints. Despite surgery, Dupuytren’s Disease may reoccur.
Splinting
Stiffness in the joints of the affected fingers can be normal after surgical treatment of Dupuytren’s disease. A thermoplastic splint will often be required to help keep the fingers straight after surgery. The type of splint required may vary depending on the severity of the condition. Your therapist or surgeon will determine which type will be most beneficial for you.
Swelling
Following surgery, it is very common to experience swelling in the hand. It is important that this is treated because swelling can interfere with wound healing and can cause finger stiffness. Post-operative swelling can be managed in a number of different ways including elevation, ice and compression. Your therapist may recommend a compressive bandage or glove. Retrograde massage is another technique utilised to reduce swelling. It involves slowly stroking the fluid down the fingertips, towards the wrist and forearm. Your therapist will teach you this technique if they would like you to begin this.
Scar Management
Once the wound has healed, scar management can commence. Scar tissue can take several months to mature and it is natural for the scar to become more thick, red and hard after surgery to treat Dupuytren’s disease.
Scar management involves:
- Massage: use small, firm, circular movements across the grain of the scar. Use a plain, non-perfumed cream such as vitamin E cream, Sorbolene cream, or Scarless Healer. Perform 4 times a day for 5-10 minutes.
- Silicone: this is a gel sheet that can help to keep your scar flat and soft and can be worn at night, while you sleep.
- Desensitisation: involves massage, exposing the scar to different textures (such as your bath towel, or Velcro), tapping the scar with your finger and using the hand as normally as possible. Doing these activities will help to make your scar less sensitive.
Exercise
Your therapist will advise you about the exercises you can do to restore the movement of the joints in your hand. Initially, you will be required to make a fist and straighten your fingers out. Once the sutures have been removed, you may commence on a regime of squeezing a rolled up sock or sponge in warm, salty water for 10 minutes, 3 – 4 times a day. This is a good way to get your hand moving again after surgery. The water warms and soothes the hand during the initial rehabilitation phase. More vigorous exercises will be prescribed as your tolerance improves. Specific exercises will be provided to enhance the motion of each individual joint of the fingers, thumb and wrist. It is important that these exercises are followed diligently to improve the post-surgical outcomes.
Strengthening
Resumption of normal activities is very important in restoring hand function and strength and so it is encouraged at every opportunity (e.g. pegging clothes on the line, brushing teeth). If your hand is weak after surgery, your hand therapist may provide you with a home strengthening program, including theraputty to help regain and improve hand strength.
If you have any questions about your hand, please contact us on 5500 5617.
References
- Abbott K, et al: A review of attitudes to splintage in Dupuytren’s contracture. J hand Surg 12B:326, 1987.
- Arem AJ, Madden JW: Effects of stress on healing wounds: 1. Intermittent noncyclical tension, J Surg Res 20(2): 93 – 102, 1976.
- Bisson, M.A, Mudera, V., McGrouther, D.A, Grobbelaar, A.O. The contractile properties and responses of tensional loading of Dupuytren’s disease. Derived fibroblasts are altered: A cause of the contracture? J of the American society of Plastic Surgeons 113(2): 611-621.
- Brand PW: Mechanical factors in joint stiffness and tissue growth, J Hand Ther 8 (2):91-6, 1995.
- Draviaraj, K.P. & Chakrabarti, I Functional outcome after surgery for Dupuytren’s contracture. J of Hand Surg :29A. 5 804-808.
- Glasgow C, Wilton J, Tooth L. Optimal daily total end range time for contracture: Resolution in hand splinting. J Hand Ther. 16:207-218, 2003.
- Hunter, Mackin, Callahan. Rehabilitation of the Hand (fifth edition) Mosby 2002
- Evans, R.B., Dell, P.C. and Biolkowski, P. A Clinical report of the effect of Mechanical stress of Functional results after Fasciectomy for Dupuytren’s contracture. J Hand Ther 15: 331-339, 2002.
- Jain AS, Mitchell C, Carus DA: A simple inexpensive post-operative management regime following surgery for Dupuytren’s contracture, J Hand Surg 13B:259, 1988.
- Peterson-Bethea D: A static progressive splint for Dupuytren’s release, J Hand Ther 10, :312, 1997.
- Prosser, R & Conolly, W.B. Complications following surgical treatment for Dupuytren’s contracture J of Hand Ther 9: 344-348, 1996.
- Prosser R. Splinting in the management of proximal interphalangeal joint flexion contracture, J Hand Ther 9(4):378-86, 1996.
- Smith P., Breed, D. Central Slip Attenuation in Dupuytren’s contracture: A cause of persistent flexion of the proximal interphalangeal joint. J Hand Surg 19A 5:840 –843 1994.
- Rivers K, et al: Severe contractures of the proximal interphalangeal joint in Dupuytren’s disease: results of a prospective trial of correction and dynamic extension splinting. J Hand Surg 17A:1153- 1158, 1992.
- Cheng, H. S., Hung, L. K., Tse, W. L., & Ho, P. C. Needle aponeurotomy for Dupuytren’s Contracture. Journal of Orthopaedic Surgery 16(1):88-90, 2008.