Management of Boutonniere Deformities
A Boutonniere Deformity in the finger is due to a disruption of the Central Slip, which is a key component of the extensor mechanism at the Proximal Interphalangeal Joint (PIPJ).1
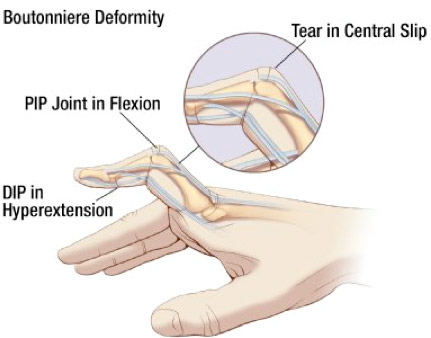
The balance between the extensor mechanism over the PIPJ and the flexors is disrupted. As the deformity progresses, the PIPJ is pulled into flexion by the Flexor Digitorum Superficialis (FDS).
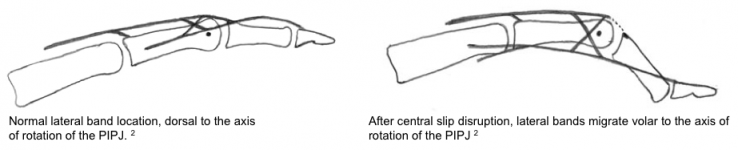
As the Central Slip becomes incompetent, the action of the Lumbrical and Interosseous muscles are diverted entirely through the Lateral Bands.2 Over time, these Lateral Bands migrate volarly and contract. This, combined with shortening of the Oblique Retinacular Ligaments, causes hyperextension at the Distal Interphalangeal Joint (DIPJ).
Assessment
These injuries should be assessed accurately and closely monitored. Patients will present with the following:
- Pain and tenderness over the dorsum of the PIPJ
- Oedema surrounding the PIPJ
- An inability to actively extend the PIPJ completely. This can be assessed using the Elson Test. From a fully flexed position, with the Metacarpophalangeal Joint (MCPJ) in neutral, the patient tries to actively extend the PIPJ, with all other fingers flexed, against gravity and then against resistance.
- For an established Boutonniere Deformity, the PIPJ is flexed and the DIPJ hyper-extended. The flexed position of the PIPJ may or may not be corrected passively.
Management
Early intervention has shown to be the most effective treatment in the prevention of joint contractures, such as Boutonniere Deformities.3 The basis of non-operative management of Boutonniere Deformities is splinting.
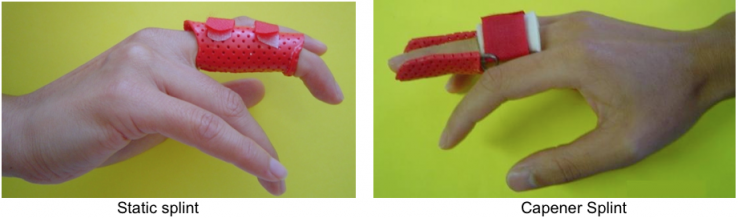
If a patient presents acutely with a closed Central Slip injury, full-time extension splinting of the PIPJ for six weeks has been recommended, with a further six weeks of night splinting.4 A static thermoplastic splint isolates the PIPJ in extension and allows for movement of the DIPJ. DIPJ flexion exercises, with the PIPJ held in extension, promotes pull through of the Lateral Bands dorsally from the volar subluxed position.
If early intervention was not initiated and a Fixed Flexion Deformity (FFD) has developed, mobilising splinting is recommended. A dynamic extension splint, known as a capener splint, is typically fabricated. It is a spring wire, three-point extension splint. It is designed to apply a small force to hold the joint at the end available extension range of movement (ROM), for long periods of time.5,6
At Gold Coast Hand Therapy, we custom make static and dynamic thermoplastic splints as described.
Surgical Intervention
A variety of surgical techniques are available for Central Slip injuries and correction of Boutonniere Deformities, if indicated. Please discuss this with a surgeon.
In our clinical experience, Hand Therapy including splinting prior to reconstruction surgery has shown to improve the post-operative outcome. This is performed at the recommendation of the treating surgeon.
1. Haerle M, Lotter O, Mertz I, Buschmeier N. [The traumatic boutonnière deformity]. Orthopade. Dec 2008;37(12):1194-201
2. Likes, R. (2010) Boutonniere Deformity. Retrieved April 19, 2011, from http://emedicine.medscape.com/article/1238095-overview#showall
3. Glasgow C, Tooth L, Fleming J. Mobilizing the Stiff Hand: Combining Theory and Evidence to Improve Clinical Outcomes. J Hand Ther. 2010;23:392-401.
4. Matzon J, Bozentka D. Extensor Tendon Injuries. JHS. 2010;35A:854-861
5. Wilton JD. Biomechanical principles of design, fabrication and application. In:Wilton J (ed). Hand Splinting. London, UK: WB Saunders Company Ltd, 1997. pp. 31–9.
6. Colditz JC. Therapist’s management of the stiff hand. In: Hunter JM, Mackin EJ, Callahan AD, Skirven TM, Schneider LH, Osterman AL (eds). Rehabilitation of the Hand and Upper Extremity. 5th ed. St Louis: Mosby, 2002. pp. 1021–49.