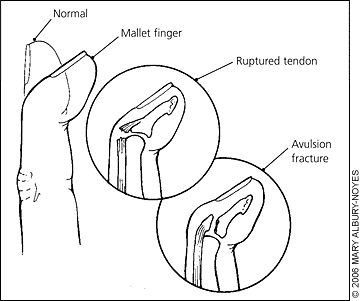
What is a mallet finger?
Mallet finger is usually caused by a sudden blow to the tip of your finger (or thumb) that then results in being unable to straighten the tip of your finger. The sudden force to the tip of the finger has caused the tendon to rupture (tendinous mallet injury) or the tendon and a piece of bone has been pulled away (bony mallet injury), resulting in there being no mechanism to pull the finger back straight.
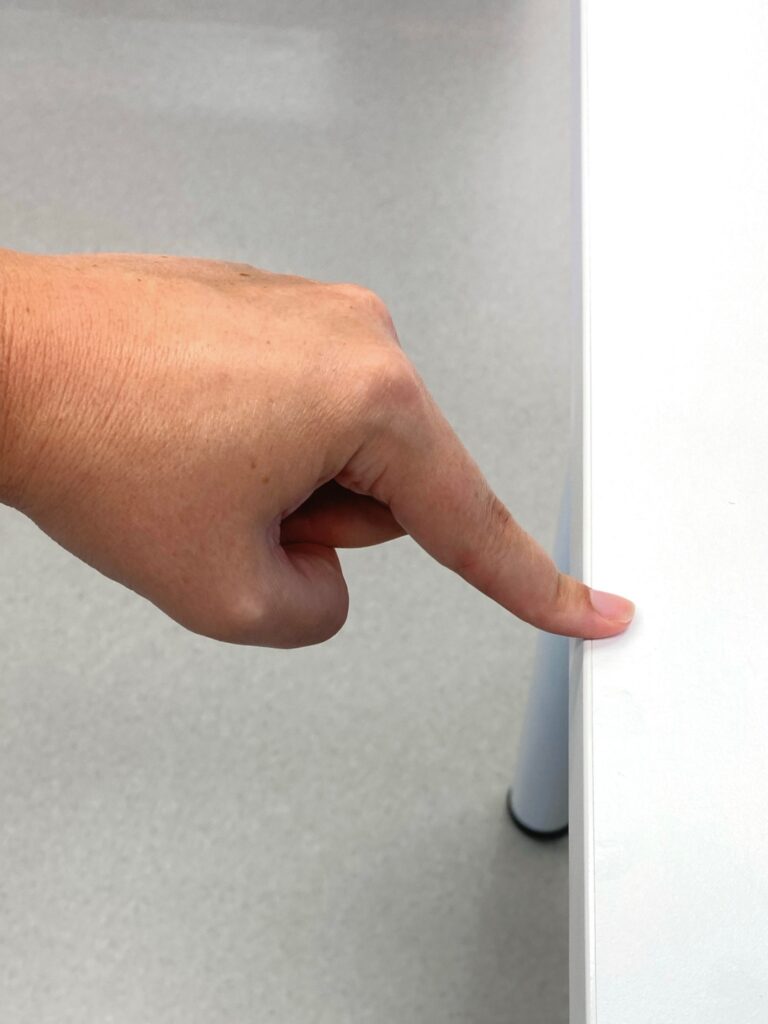
How do I know I have a mallet finger injury?
The tip finger joint can be pushed straight but you cannot hold that position when the support is removed.
You may also have pain, tenderness, and swelling at this joint immediately after the injury or soon after.
Can a mallet finger heal on its own?
If you have a mallet finger, it needs to be treated, it will not heal on its own. We strongly advise against self-managing by reinforcing the joint at home due to risk of pressure areas and to protect skin integrity. You should always see a hand therapist.
I have a mallet finger or thumb injury, what should I do next?
If you have a fingertip that will not straighten on its own, you should immediately consult with a hand therapist. They can commence splinting and guide you through the next stages of your management. It is also beneficial to have Xray imaging of the finger so it can be identified if you have a bony or tendinous mallet injury and if a specialist or surgical review is required.
Treatment of a mallet injury?

A good understanding of the treatment expectations is very important in the management of a mallet injury as splinting compliance is vital in a good outcome.
- Your therapist will fabricate a small custom moulded thermoplastic splint to be worn over the back of your finger and secured with small strapping tape.
- The splint must be worn FULL TIME throughout the duration of your splinting plan (6-8 weeks), removing only for hygiene and if the fleece lining needs to be changed.
- When the splint is removed for these times, your fingertip must remain straight and supported by your other hand or the tabletop and CANNOT bend. If the fingertip bends forwards the healing will be undone
- and splinting will likely recommence from week one.
- You will be encouraged to maintain range of movement of the unaffected joints of the finger.
In some cases, surgical intervention may be required if the bone fragment that has been pulled away with the tendon is a large fragment or if there is poor joint alignment. Surgery may also be considered if wearing a splint is difficult or in the rare case that there is a poor outcome following 6-8 weeks splinting. Your hand therapist or hand surgeon would discuss any of these outcomes/recommendations further with you as required.
How long will I wear my splint for?
- Bony mallet injury (avulsion fracture) = 6 weeks full time
- Tendinous mallet injury = 8 weeks full time
- It is advised to continue night-time splinting ongoing for up to 3months post injury to prevent any ‘lag’/drooping of this tip joint.
Can I continue to play sport with a mallet injury?
Returning to sport does increase the risk of re-injury or the potential for your splint to loosen in high impact activity. If you cannot have a break from your chosen sports, it is important to discuss this with your hand therapist to ensure an appropriate plan can be established to minimise the risk of returning to activity. Remember though, your splint MUST be worn full time and therefore it must be allowed within the guidelines of the activity you wish to participate in.
I have now finished the 6-8 weeks of splinting, what next?
- Your hand therapist will have scheduled a follow up appointment at this point to remove the splint and ensure you can now straighten your finger with support removed.
- You will be advised to continue night-time splinting as mentioned above and will likely require splinting ongoing for ‘at risk’ activities (for example playing sport) but your therapist will guide you with this.
- Your finger may not be completely straight after this injury, this is always the therapy goal however there can still be a slight bend at the tip no matter how diligent you are with your splinting.
- When your splint is removed, the tip of your finger will be stiff bending, this is expected. It is very important that you do not force your finger to bend, your movement will gradually improve as you start to use your hand normally and with the exercises that your hand therapist gives you.
How many times will I need to see my hand therapist?
This can vary depending on how confident you are with your splint changes, skin integrity, joint movement, and also strength once the splint has been removed (or wound management should surgical repair be required).
Generally, on average in a typical presentation 2-4 appointments will be required.
- Initial consult: splint fabrication and treatment plan established
- Appointment 2: at approximately 3 weeks of splinting (if needed) for a splint check that could need to be remoulded to accommodate a reduction in swelling and to review technique of splint changes.
- Appointment 3: at 6-8 weeks of splinting depending on tendinous or bony mallet injury to wean from splint and to establish home exercise program (movement exercises and graded strengthening regime).
- Appointment 4: likely final consult to review progress, assess strength and range of movement and educate regarding ongoing self-management.
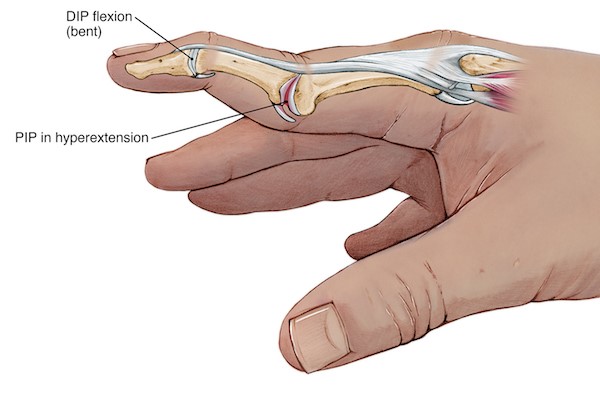
Precautions/what to be aware of moving forward:
It would be advised that should the lag/drop in the tip of the finger return or increase after being discharged from therapy that you should return to see your hand therapist. If left untreated or through failed conservative management, mallet finger can lead to a swan neck deformity. A swan neck deformity is from PIP joint hyper extension and DIP joint flexion due to an imbalance in the soft tissue structures (see picture on the Right). A referral to a hand surgeon for opinion and potential management may be recommended at this stage.
Written by: Mikayla Pope – Occupational Therapist – Robina